

Thyroidectomy
What is Thyroidectomy?
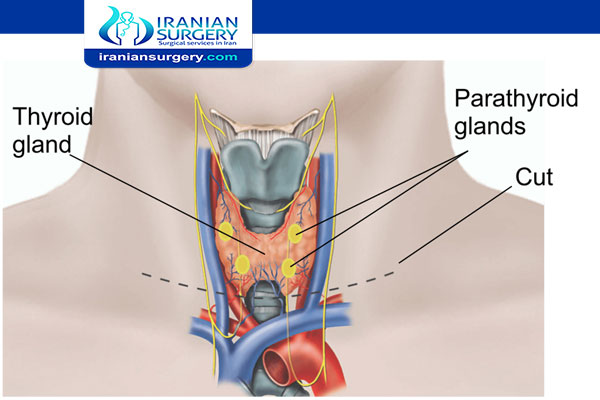
Thyroidectomy is the surgical removal of all or part of your thyroid gland. Your thyroid is a butterfly-shaped gland located at the base of your neck. It produces hormones that control every aspect of your metabolism, from your heart rate to how quickly you burn calories.
Thyroidectomy is used to treat thyroid disorders, such as cancer, noncancerous enlargement of the thyroid (goiter) and overactive thyroid (hyperthyroidism).
How much of your thyroid gland is removed during thyroidectomy depends on the reason for surgery. If you need only part of your thyroid removed (partial thyroidectomy), your thyroid may work normally after surgery. If your entire thyroid is removed (total thyroidectomy), you need daily treatment with thyroid hormone to replace your thyroid's natural function.
________________________________________________________________________________________
Plan your Thyroidectomy surgery in Iran with the Best surgeon.
Iranian Surgery is a medical tourism company in Iran that cooperates with the best surgeon, specialists and hospitals in Iran and offers world-class treatments at an affordable cost.
_________________________________________________________________________________________
Read more about : Coronary artery bypass surgery (CABG) success story
Read more about : Leg lengthening surgery success story in Iran
Read more about : Total knee replacement surgery success story in Iran
Read more about : Kidney transplant in Iran success story in Iran
Read more about : Cancer treatment success story in Iran
Read more about : Sex reassignment surgery success story
Read more about : Parkinson's disease treatment success story
Read more about : Heart Bypass Surgery
Read more about : Types of Thyroidectomy
Before Thyroidectomy Surgery
Why it's done
Your doctor may recommend a thyroidectomy if you have conditions such as:
. Thyroid cancer. Cancer is the most common reason for thyroidectomy. If you have thyroid cancer, removing most, if not all, of your thyroid will likely be a treatment option.
. Noncancerous enlargement of the thyroid (goiter). Removing all or part of your thyroid gland is an option if you have a large goiter that is uncomfortable or causes difficulty breathing or swallowing or, in some cases, if the goiter is causing hyperthyroidism.
. Overactive thyroid (hyperthyroidism). Hyperthyroidism is a condition in which your thyroid gland produces too much of the hormone thyroxine. If you have problems with anti-thyroid drugs and don't want radioactive iodine therapy, thyroidectomy may be an option.
. Indeterminate or suspicious thyroid nodules. Some thyroid nodules can't be identified as cancerous or noncancerous after testing a sample from a needle biopsy. Doctors may recommend that people with these nodules have thyroidectomy if the nodules have an increased risk of being cancerous.
Read more about : Thyroid Cancer Treatment
Read more about : Cancer treatment
Risks and Complications
Thyroidectomy is generally a safe procedure. But as with any surgery, thyroidectomy carries a risk of complications.
Potential complications include:
. Hemorrhage (bleeding) beneath the neck wound — if this occurs, the wound bulges and the neck swells, possibly compressing structures inside the neck and interfering with breathing. This is an emergency.
. Thyroid storm — if a thyroidectomy is done to treat a very overactive gland, there may be a surge of thyroid hormones into the blood. This is a very rare complication because medications are given before surgery to prevent this problem.
. Hypoparathyroidism — if the parathyroid glands cannot be saved or are damaged during surgery, the person may not be able to make enough parathyroid hormone. Parathyroid hormone helps keep blood calcium levels in the normal range. Low parathyroid hormone output causes low blood calcium levels.
. Injury to the recurrent laryngeal nerve — because this nerve supplies the vocal cords, injury can lead to vocal cord paralysis and can produce a husky voice, either short term or long term.
. Injury to a portion of the superior laryngeal nerve — if this occurs, patients who sing may not be able to hit high notes, and the voice may lose some projection.
. Wound infection — any surgical incision carries a risk that the site could become infected.
. Airway obstruction caused by bleeding.
Read more about: prostate cancer treatments pros and cons
Read more about: Thyroidectomy scar
How you prepare
. Food and medications
If you have hyperthyroidism, your doctor may prescribe medication — such as an iodine and potassium solution — to control your thyroid function and lower the bleeding risk after surgery.
You may need to avoid eating and drinking for a certain period of time before surgery, as well, to avoid anesthesia complications. Your doctor will provide specific instructions.
. Other precautions
Before your scheduled surgery, ask a friend or loved one to help you get home after the procedure. Be sure to leave jewelry and valuables at home.
What you can expect
Before the procedure
Surgeons typically perform thyroidectomy during general anesthesia, so you won't be conscious during the procedure. The anesthesiologist or anesthetist gives you an anesthetic medication as a gas — to breathe through a mask — or injects a liquid medication into a vein. A breathing tube will then be placed in your trachea to assist breathing throughout the procedure.
The surgical team places several monitors on your body to help make sure that your heart rate, blood pressure and blood oxygen remain at safe levels throughout the procedure. These monitors include a blood pressure cuff on your arm and heart-monitor leads attached to your chest.
Read more about: Common side effects of thyroid cancer treatment:
During Thyroidectomy Surgery
Types of thyroidectomy
The various types of thyroidectomy include:
. Partial Thyroid Lobectomy (a rare procedure) — only part of one thyroid lobe is removed. This operation is not performed very often because there are not many conditions which will allow this limited approach. Additionally, a benign lesion must be ideally located in the upper or lower portion of one lobe for this operation to be a choice.
. Thyroid lobectomy — all of one thyroid lobe is removed. This is typically the "smallest" operation performed on the thyroid gland. It is performed for solitary dominant nodules, which may be thyroid cancer or those which are indeterminate following fine needle biopsy. This surgery may also be appropriate for follicular adenomas, solitary hot or cold nodules, or goiters which are isolated to one lobe (not common).
. Thyroid lobectomy with isthmusectomy — all of one thyroid lobe is removed, together with the section between the two lobes (called the thyroid isthmus). This simply means removal of a thyroid lobe and the isthmus (the part that connects the 2 lobes). This removes more thyroid tissue than a simple lobectomy, and is used when a larger margin of tissue is needed to assure that the "problem" has been removed. Appropriate for those indications listed under thyroid lobectomy as well as for Hurthle cell tumors, and some very small and non-aggressive thyroid cancers.
. Subtotal thyroidectomy — One thyroid lobe, the isthmus and part of the second lobe are removed. This operation is typical for small, non-aggressive thyroid cancers. Also a common operation for goiters that are causing problems in the neck or even those which extend into the chest (substernal goiters).
. Total thyroidectomy — the entire thyroid gland is removed. It is the operation of choice for all thyroid cancers which are not small and non-aggressive in young patients. Many surgeons prefer complete removal of thyroid tissue for all the different types of thyroid cancer.
Read more about: Herniated Disk Treatment
Read more about: Coronary Angiography
During the procedure
Once you're unconscious, the surgeon makes a cut (incision) low in the center of your neck. It can often be placed in a skin crease where it will be difficult to see after the incision heals. All or part of the thyroid gland is then removed, depending on the reason for the surgery.
If you're having thyroidectomy as a result of thyroid cancer, the surgeon may also examine and remove lymph nodes around your thyroid. Thyroidectomy usually takes one to two hours. It may take more or less time, depending on the extent of the surgery needed.
There are several approaches to thyroidectomy, including:
. Conventional thyroidectomy. The majority of people will likely be candidates for this procedure. In a conventional thyroidectomy, a 3- to 4-inch incision will be made through the skin in the low collar area of your neck (the lower front portion of your neck, above the collarbones and breast bone). Next, a vertical cut will be made through the strap-like muscles located just below the skin, and these muscles will be spread aside to reveal the thyroid gland and other deeper structures. Then, all or part of your thyroid gland will be cut free from surrounding tissues and removed.
During the entire procedure, the surgeon will pay attention to the location of the parathyroid glands (two pairs of small glands located near the thyroid). The surgeon will focus on preserving them, if possible. After your thyroid gland is removed, one or two stitches will be used to bring your neck muscles together again. Then the deeper layer of your incision will be closed with stitches, and your skin will be closed with sterile paper tapes. A small suction catheter (tube) may be inserted near the area of your incision to drain any blood accumulated inside your neck.
Following surgery, you will be taken to a recovery room, where you will be monitored for several hours until you are stable enough to return to your hospital room. After about 24 hours, the suction catheter will be removed from your neck if it was needed. Most patients go home one or two days after the surgery.
. Transoral thyroidectomy. This approach avoids a neck incision by using an incision inside the mouth.
. Endoscopic thyroidectomy. A viewing instrument called an endoscope and small surgical instruments will be inserted into your neck through three or four small incisions. Each incision is about 3 millimeters to 5 millimeters long (less than ¼ inch). Then the surgeon will use a tiny camera on the endoscope to guide the instruments and remove your thyroid tissue. At the end of the procedure, your neck incisions will be closed with tiny stitches or surgical tape.
After Thyroidectomy Surgery
After the procedure
After surgery, you're moved to a recovery room where the health care team monitors your recovery from the surgery and anesthesia. Once you're fully conscious, you'll be moved to a hospital room.
Some people may need to have a drain placed under the incision in the neck. This drain is usually removed the morning after surgery.
After thyroidectomy, a few people may experience neck pain and a hoarse or weak voice. This doesn't necessarily mean there's permanent damage to the nerve that controls the vocal cords. These symptoms are often short-term and may be due to irritation from the breathing tube that's inserted into the windpipe during surgery, or be a result of nerve irritation caused by the surgery.
After thyroidectomy, you will need periodic blood tests to measure your thyroid hormone levels. Calcium and phosphorus levels are checked to evaluate the function of your parathyroid glands, which sometimes are damaged during thyroid surgery. If all of your thyroid gland was removed, you can expect to take thyroid supplements for the rest of your life.
You'll be able to eat and drink as usual after surgery. Depending on the type of surgery you had, you may be able to go home the day of your procedure or your doctor may recommend that you stay overnight in the hospital.
When you go home, you can usually return to your regular activities. Wait at least 10 days to two weeks before doing anything vigorous, such as heavy lifting or strenuous sports.
It takes up to a year for the scar from surgery to fade. Your doctor may recommend using sunscreen to help minimize the scar from being noticeable.
When to call a Doctor
Once you return home from the hospital, call your doctor immediately if:
. You develop a fever.
. Your incision or any part of your neck becomes red, tender or swollen.
. Your voice seems to be hoarse, husky or weak.
. You develop symptoms of a low blood calcium level, such as numbness around your mouth, tingling in your extremities, or spasms in your feet, hands or face.
Results
The long-term effects of thyroidectomy depend on how much of the thyroid is removed.
. Partial thyroidectomy
If only part of your thyroid is removed, the remaining portion typically takes over the function of the entire thyroid gland. So you might not need thyroid hormone therapy.
. Complete thyroidectomy
If your entire thyroid is removed, your body can't make thyroid hormone. Without replacement, you'll develop signs and symptoms of underactive thyroid (hypothyroidism). Therefore, you'll need to take a pill every day that contains the synthetic thyroid hormone levothyroxine (Synthroid, Unithroid, others).
This hormone replacement is identical to the hormone normally made by your thyroid gland and performs all of the same functions. Your doctor will test your blood to know how much thyroid hormone replacement you need.