

Moyamoya disease
What is the cause of Moyamoya disease?
What are the symptoms of Moyamoya disease?
Moyamoya disease life expectancy
Is Moyamoya disease hereditary?
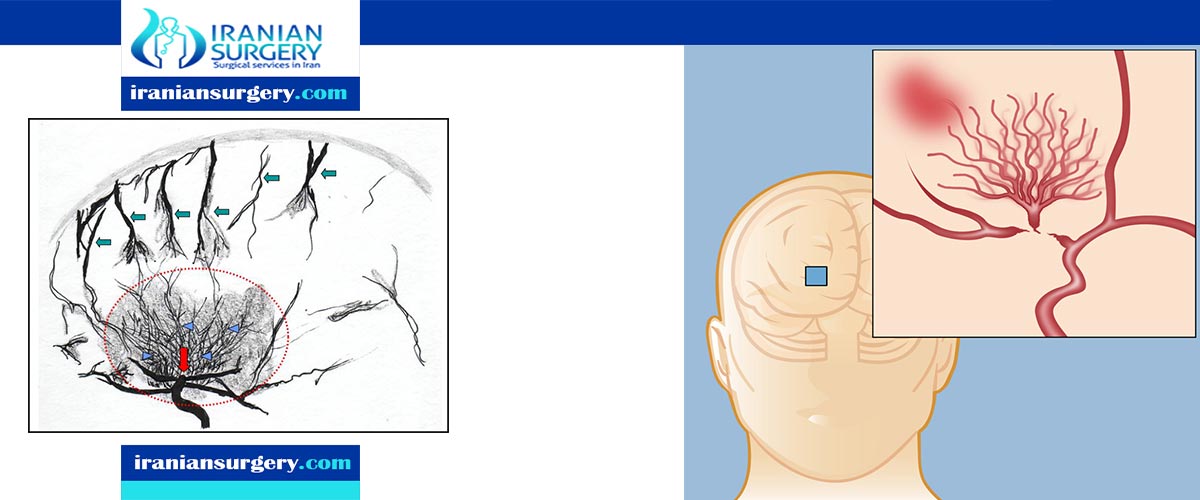
Moyamoya disease is a disease in which certain arteries in the brain are constricted. Blood flow is blocked by the constriction, and also by blood clots (thrombosis).
A collateral circulation develops around the blocked vessels to compensate for the blockage, but the collateral vessels are small, weak, and prone to bleeding, aneurysm and thrombosis. On conventional X-ray angiography, these collateral vessels have the appearance of a "puff of smoke".
When Moyamoya is diagnosed by itself, with no underlying correlational conditions, it is diagnosed as Moyamoya disease. This is also the case when the arterial constriction and collateral circulation are bilateral. Moyamoya syndrome is unilateral arterial constriction, or occurs when one of the several specified conditions is also present. This may also be considered as Moyamoya being secondary to the primary condition. Mainly, occlusion of the distal internal carotid artery occurs. On angiography, a "puff of smoke" appearance is seen, and the treatment of choice is surgical bypass.
Read more about : Parkinson’s disease treatment
Read more about : What is considered a large arachnoid cyst?
What is the cause of Moyamoya disease?
The exact cause of Moyamoya disease is unknown. Moyamoya disease is most commonly seen in Japan, Korea and China, but it also occurs in other parts of the world. Researchers believe the greater prevalence in these Asian countries strongly suggests a genetic factor in some populations.
Moyamoya is also associated with certain conditions, such as Down syndrome, sickle cell anemia, neurofibromatosis type 1 and hyperthyroidism.
Risk factors
Though the cause of Moyamoya disease is unknown, certain factors may increase your risk of having the condition, including:
- Being of Asian descent. Moyamoya disease is found all over the world, but it's more common in East Asian countries, especially Korea, Japan and China. This may possibly be due to certain genetic factors in those populations. This same higher prevalence has been documented among Asians living in Western countries.
- Having a family history of Moyamoya disease. If you have a family member with Moyamoya disease, your risk of having the condition is 30 to 40 times higher than that of the general population — a factor that strongly suggests a genetic component.
- Having a certain medical condition. Moyamoya disease sometimes occurs in association with another disorder, including neurofibromatosis type 1, sickle cell disease and Down syndrome, among many others.
- Being female. Females have a slightly higher incidence of Moyamoya disease.
- Being young. Though adults can have Moyamoya disease, children younger than 15 years old are most commonly affected.
What are the symptoms of Moyamoya disease?
- Recurring transient ischemic attacks (TIAs or “mini-strokes”)
- Epilepsy
- Stroke: Ischemic stroke (due to blockage) or hemorrhagic stroke (bleeding)
- Hemiparesis: weakness or paralysis on one side of the body
- Progressive difficulty in thinking and remembering due to repeated strokes and bleeding
In diagnosing Moyamoya disease, the doctor may recommend an electroencephalogram, or EEG, which may show a characteristic electrical pattern when the person is asked to breathe heavily.
Read more about Spinal Fusion Surgery
Moyamoya disease diagnosis
Cerebral angiography is the gold standard of diagnosing Moyamoya disease and its progression. According to the Suzuki's system, it can be classified into: six stages:
- Stage 1 Narrowing of carotid fork
- Stage 2 Initiation of the Moyamoya and dilatation of intracranial main arteries
- Stage 3 Intensification of the Moyamoya and defects of the anterior cerebral artery and middle cerebral artery
- Stage 4 Minimization of the Moyamoya and defects of the posterior cerebral artery
- Stage 5 Reduction of the Moyamoya and development of external carotid artery collaterals
- Stage 6 Disappearance of the Moyamoya and circulation only via external cerebral artery and vertebral artery
Magnetic resonance angiography (MRA) is also useful in diagnosing the disease with good correlation with Suzuki's grading system.
Proliferation of smooth muscle cells in the walls of the Moyamoya-affected arteries has been found to be representative of the disease. A study of six autopsies of six patients who died from Moyamoya disease lead to the finding that there is evidence that supports the theory that there is a thickening, or proliferation, of the innermost layer of the vessels affected by Moyamoya. These vessels are the ACA (anterior cerebral artery), MCA (middle cerebral artery), and ICA (internal carotid artery). The occlusion of the ICA results in concomitant diminution of the "puff-of-smoke" collaterals, as they are supplied by the ICA.
Often nuclear medicine studies such as SPECT (single photon emission computerized tomography) are used to demonstrate the decreased blood and oxygen supply to areas of the brain involved with Moyamoya disease. Conventional angiography provides the conclusive diagnosis of Moyamoya disease in most cases and should be performed before any surgical considerations.
Read more about Arachnoid Cyst Treatment
Associated biomarkers
Smith (2015) conducted a study that looked into specific biological markers that correlate to Moyamoya disease. Some of the categories of these biomarkers include phenotypes - conditions commonly related to Moyamoya, radiographical markers for the diagnosis of Moyamoya, and proteins as well as cellular changes that occur in cases of Moyamoya.
Similar to Moyamoya disease, there are conditions that are closely associated with Moyamoya disease. Some of the more common medical conditions that are closely associated with Moyamoya disease include trisomy 21 (Down's Syndrome), sickle cell disease, and neurofibromatosis type 1. There is also evidence that identifies hyperthyroidism and congenital dwarfing syndromes as two of the more loosely associated syndromes that correlate with the possibility of being diagnosed with Moyamoya disease later in life.
There is also research that has shown that certain radiographic biomarkers that lead to the diagnosis of Moyamoya disease have been identified. The specific radiographic markers are now considered an acceptable key component to Moyamoya Disease and have been added to the International Classification of Diseases (ICD). These biomarkers of Moyamoya are "stenosis of the distal ICA's up to and including the bifurcation, along with segments of the proximal ACA and MCA...dilated basal collateral vessels must be present" Some other common findings that have not been added to the classification index of those with Moyamoya disease which are found using radiography involve very distinct changes in the vessels of the brain. These changes include newly formed vessels made to compensate for another change noted, ischemia and cerebrovascular reserve, both found on MRI. Functional changes include evidence of ischemia in vessels of the brain (ICA, ACA, MCA, specifically). It is important to also note that the radiographic biomarkers, in order to be classified as Moyamoya disease, all findings must be bilateral. If this is not the case and the findings are unilateral, it is diagnosed as Moyamoya Syndrome.
There are also several protein biomarkers that have been linked to the Moyamoya disease diagnosis. Although the sample size of the studies performed are small due to the rarity of the disease, the findings are indicative of a correlation between the disease and several specific protein biomarkers. Other studies have confirmed the correlation of Moyamoya and adhesion molecule 1 (ICAM-1) being increased as compared to normal vascular function counterparts. Furthermore, it has been concluded that the localization of inflammatory cells suggests that the inflammation stimulus iteself may be responsible for the proliferation and occlusion in the ICA, ACA, and MCA found in those with Moyamoya disease.
Read more about: Vascular surgery
Moyamoya disease treatment
There is no cure for this disease. Drugs such as antiplatelet agents (including aspirin) are usually given to prevent clots, but surgery is usually recommended. Since Moyamoya tends to affect only the internal carotid artery and nearby sections of the adjacent anterior and middle cerebral arteries, surgeons can direct other arteries, such as the external carotid artery or the superficial temporal artery to replace its circulation. The arteries are either sewn directly into the brain circulation, or placed on the surface of the brain to reestablish new circulation after a few weeks.
There are many operations that have been developed for the condition, but currently the most favored are the in-direct procedures EDAS, EMS, and multiple burr holes and the direct procedure STA-MCA. Direct superficial temporal artery (STA) to middle cerebral artery (MCA) bypass is considered the treatment of choice, although its efficacy, particularly for hemorrhagic disease, remains uncertain. Multiple burr holes have been used in frontal and parietal lobes with good neovascularisation achieved.
The EDAS (encephaloduroarteriosynangiosis) procedure is a synangiosis procedure that requires dissection of a scalp artery over a course of several centimeters and then making a small temporary opening in the skull directly beneath the artery. The artery is then sutured to a branch of the middle cerebral artery on the surface of the brain and the bone is replaced.
In the EMS (encephalomyosynangiosis) procedure, the temporalis muscle, which is in the temple region of the forehead, is dissected and through an opening in the skull placed onto the surface of the brain.
In the multiple burr holes procedure, multiple small holes (burr holes) are placed in the skull to allow for growth of new vessels into the brain from the scalp.
In the STA-MCA procedure, the scalp artery (superficial temporal artery or STA) is directly sutured to an artery on the surface of the brain (middle cerebral artery or MCA). This procedure is also commonly referred to as an EC-IC (External Carotid-Internal Carotid) bypass.
All of these operations have in common the concept of a blood and oxygen "starved" brain reaching out to grasp and develop new and more efficient means of bringing blood to the brain and bypassing the areas of blockage. The modified direct anastomosis and encephalo-myo-arterio-synangiosis play a role in this improvement by increasing cerebral blood flow (CBF) after the operation. A significant correlation is found between the postoperative effect and the stages of preoperative angiograms. It is crucial for surgery that the anesthesiologist have experience in managing children being treated for Moyamoya, as the type of anesthesia they require is very different from the standard anesthetic children get for almost any other type of neurosurgical procedure.
Read more about: peripheral angioplasty with vascular closure device
Is Moyamoya disease curable?
Moyamoya is a progressive disease that does not improve without treatment. While Moyamoya itself is not curable, surgery to provide alternative blood flow to the brain prevents the symptoms related to Moyamoya and can provide an excellent long term outcome with significant stroke risk reduction.
Read more about: Angioplasty in Iran
Moyamoya disease life expectancy
Mortality rates from Moyamoya disease are approximately 10% in adults and 4.3% in children. About 50-60% of affected individuals experience a gradual deterioration of cognitive function, presumably from recurrent strokes.
Is Moyamoya disease hereditary?
Moyamoya disease most commonly affects children, but adults may have the condition. Moyamoya disease is found all over the world, but it's more common in East Asian countries, especially Korea, Japan and China. This may possibly be due to certain genetic factors in those populations.
Read more about: peripheral angioplasty with vascular closure device