

Fetal Positions for Birth
Fetal Positions for Birth
What Does Fetal Positioning Mean?
The position of the baby in your uterus is called the presentation of the fetus. Throughout your pregnancy, your baby will move around in the uterus. It’s normal for your baby to be in a variety of positions during most of the pregnancy. Early on, the baby is small enough to move freely. You may have even felt this movement over the last few months. The larger the baby becomes, however, the more limited the movement becomes. As the end of the pregnancy approaches, the baby will start to move into position for birth. This typically involves flipping over so that the baby is head down in your womb. The baby will start to move down in your uterus, preparing to go through your birth canal during childbirth.
The birth canal is made up of your cervix (immediately outside of your uterus), vagina and vulva. Think of the birth canal as an expandable tunnel. During labor, your contractions work to stretch this space so that the baby can pass through it during childbirth.
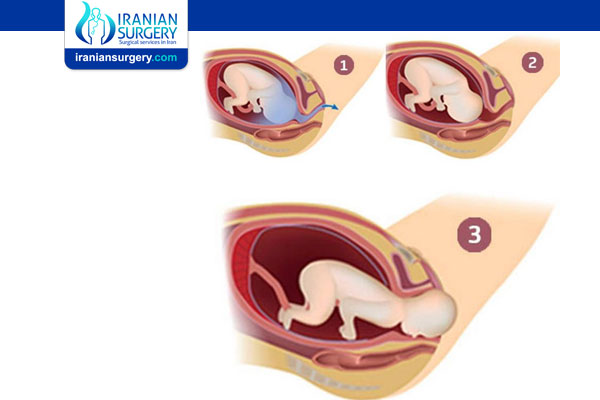
What is the most common position for childbirth?
Ideally for labor, the baby is positioned head-down, facing the mother’s back with the chin tucked to its chest and the back of the head ready to enter the pelvis. This position is called cephalic presentation. Most babies settle into this position within the 32nd to 36th weeks of pregnancy.
What other positions can the baby be in before childbirth?
Sometimes the baby doesn’t get into the perfect position before birth. There are several positions that the baby can be in and each of these positions could come with complications during childbirth. These fetal positions can include:
. Occiput or cephalic posterior position: Sometimes the baby is positioned head down as it should be, but other times it is facing the mother's abdomen. With the head in this position, the baby is looking at the ceiling. You may hear this position nicknamed sunny-side-up. This increases the chance of a painful and prolonged delivery.
. Frank breech: In a frank breech, the baby's buttocks lead the way into the birth canal. The hips are flexed, the knees extended (in front of the abdomen). This position increases the chance of forming an umbilical cord loop that could precede the head through the cervix and cause the baby to be injured during a vaginal delivery.
. Complete breech: In this position, the baby is positioned with the buttocks first and both the hips and the knees are flexed (folded under themselves). Like other breech presentations, this position increases the risk of forming an umbilical cord loop that could precede the head through the cervix and injure the baby if delivered vaginally.
. Transverse lie: The baby lies crosswise in the uterus, making it likely that the shoulder will enter the pelvis first. Most babies in this position are delivered by cesarean (C-section).
. Footling breech: Sometimes, one or both of the baby's feet are pointed down toward the birth canal. This increases the chances of the umbilical cord slithering down into the mouth of the womb, cutting off blood supply to the baby.
Is my baby at risk if it’s in a breech position?
A breech birth is when the baby is positioned with its feet down in the birth canal. While in the womb, the baby isn’t in any danger. However, in this position, the baby would be born foot first. A vaginal delivery is often a very safe form of childbirth, however, when the baby is breech, a vaginal delivery can be complicated. Because the baby’s head is larger than the bottom, there is a risk of head entrapment where the baby’s head becomes stuck in the uterus. In this situation, the baby can be difficult to deliver. Some babies in the breech position may want to come in a hurry during labor. Some providers are comfortable performing a vaginal birth as long as the baby is doing well. In many cases, your healthcare provider may recommend a cesarean birth (C-section) instead of a vaginal birth. This is a surgical procedure where an incision is made in the mother’s abdomen and the baby is removed in an operating room. There’s a lot less risk to the baby during this procedure compared to a breech vaginal birth.
Why does the position of the baby at birth matter?
During childbirth, your healthcare provider’s goal is to safely deliver your baby and ensure your well-being. If the baby is in a different position (not a cephalic presentation), this job becomes more challenging. Different fetal positions have a range of difficulties and the risks can vary depending on the position of your child.
When should my baby move into position for birth?
Typically, your baby will drop down in the uterus and move into position for birth in the third trimester. This happens in the last few weeks of your pregnancy (often between weeks 32 and 36). Your healthcare provider will check the position of the baby by touching your abdomen during your regular appointments. This will happen during most of your appointments in the third trimester. In some cases, your provider may also do an ultrasound to check the baby’s position.
Can my healthcare provider turn or reposition my baby before birth?
There are several ways that your healthcare provider can try and turn the baby before you go into labor. These methods don’t always work and sometimes, the baby can actually turn back into the wrong position again. You can actually try some of these techniques at home and they won’t harm you or your baby. They might encourage your baby to turn on its own, but there’s also a chance that nothing will happen. Even though there isn’t a guaranteed success rate, these methods are still recommended because they’re usually worth a try and could help you avoid a C-section delivery.
Methods for turning your baby can include:
. External cephalic version (ECV): ECV is one non-invasive way to turn the baby and improve your chance of having a vaginal birth. This procedure is performed on the labor and delivery unit. This procedure requires two providers where one is lifting up the baby’s buttocks in an upward position and the second provider is applying pressure through the abdominal wall to the uterus where the baby is located to rotate the baby’s head forward or backward. The best time to perform this procedure is between 36 to 38 weeks of pregnancy. Afterwards, the baby’s heart rate will be monitored to make sure it’s within normal levels. You should be able to go home after ECV.
. Changing your position: Sometimes you can encourage the baby to move by changing your position. Keep in mind that these exercises might not work. However, experts often feel that attempting these exercises won’t hurt and if there is a chance that they might encourage the baby to turn, avoiding a C-section, it’s worth trying. These positions typically involve doing yoga-like poses. Two specific movements that your provider may recommend include:
. Getting on your hands and knees and gently rocking back and forth.
. Pushing your hips up in the air while laying on your back with your knees bent and feet flat on the floor (bridge pose).
. Using stimulating sounds to encourage movement: Another thing you can try to get the baby to change position is stimulation. Music, talking, temperature changes and light could interest the baby. While in the womb, your baby can hear music, see light changes through your skin and even hear your voice as you talk. You can try placing headphone on your belly, towards the bottom, to see if this attracts your baby. Applying cool temperatures to the top of your abdomen where the baby’s head is could also promote the baby to move away and downward. Similarly to changing your position, there is no guarantee that stimulation will make your baby move, but it’s often worth a try.
A chiropractic technique, called the Webster technique, can also be used to move your hips. This is meant to allow your uterus to relax. Some providers even recommend acupuncture to help your body relax. Both of these techniques need to be done by a professional that your healthcare provider has recommended. Relaxation could promote movement in the baby and help get the baby into the best possible position for birth.
Can my baby change position on its own?
It’s always possible that your baby will reposition all on its own. In the weeks leading up to birth, the baby still has time to make adjustments and change position. Most babies find their own way into the correct position before birth.
How is the baby delivered when it’s breech or in another position?
Most birth plans begin with the idea of having a vaginal birth. Your provider will look at your medical history, the scans of your baby throughout the pregnancy and the position of the baby to pick the safest form of delivery. When the baby is in a breech position or another abnormal position, your healthcare provider may suggest a cesarean section (C-section) delivery. This is a surgical procedure where an incision is made in your lower abdomen. The baby is delivered through this opening instead of through the birth canal.
It is possible to deliver a breech baby vaginally. However, this type of birth can be much more dangerous for the baby and the risk of injury from the umbilical cord is much higher. If the cord is compressed during birth, the baby could be deprived of oxygen and this could harm the brain and nerves. The cord could also slip around the baby’s neck or arms, causing injury. Different healthcare providers have various levels of comfort with vaginal deliveries of breech babies. Talk to your provider about the risks and benefits of different types of birth for a breech baby.
Does anything increase my risk of having a dangerous fetal position?
There are several factors that could increase the risk of a fetal position like a breech presentation. These can include:
. Going into labor too early and having a premature baby. In this case, the baby may not have had time to turn in preparation for birth yet.
. Having issues with the placenta. If the placenta is either attached too low in the uterus (a condition called placenta previa) or disconnects from the uterus before birth, it could prevent the baby from turning and getting into the right position for birth.
. Having a multiple pregnancy. When there’s more than one baby in the uterus, it can be difficult for each baby to get into position. The limited space creates problems as the babies develop throughout the pregnancy.
. Having a uterus that is shaped differently than normal. The uterus is typically shaped like an upside-down pear. When it’s shaped abnormally or has fibroids (growths that can vary in size), there might not be enough shape for a full-grown baby to move into position for birth.
How can I prepare for complications like a breech delivery?
Learning that your baby is in a breech or other complicated position before birth can add to the anxiety that often surrounds childbirth. It’s alright to have concerns and questions about what this means for your birth experience. You may have developed a birth plan during your pregnancy. A birth plan is an ideal plan for your labor and delivery. These plans can be very helpful as a tool. Take your birth plan to an appointment and talk to your healthcare provider about what you are picturing for your labor and delivery. Your provider can help guide you through not only the ideal plan, but an emergency plan. Remember, things can change quickly during childbirth. Having a C-section may not be a part of your birth plan. However, the goal is to safely deliver your child and protect your health. Talk to your healthcare provider about questions and any concerns you might have about your baby’s position.
Source:
. https://my.clevelandclinic.org/health/articles/9677-fetal-positions-for-birth