

Root canal treatment
Root canal treatment
Root canal treatment (also known as endodontic therapy, endodontic treatment, or root canal therapy) is a treatment sequence for the infected pulp of a tooth which results in the elimination of infection and the protection of the decontaminated tooth from future microbial invasion. Root canals, and their associated pulp chamber, are the physical hollows within a tooth that are naturally inhabited by nerve tissue, blood vessels and other cellularentities. Together, these items constitute the dental pulp. Endodontic therapy involves the removal of these structures, the subsequent shaping, cleaning, and decontamination of the hollows with small files and irrigating solutions, and the obturation (filling) of the decontaminated canals. Filling of the cleaned and decontaminated canals is done with an inert filling such as gutta-percha and typically a eugenol-based cement. Epoxy resin is employed to bind gutta-percha in some root canal procedures. Endodontics includes both primary and secondary endodontic treatments as well as periradicular surgery which is generally used for teeth that still have potential for salvage.
Read more about : Gingivectomy

Root canal procedure: unhealthy or injured tooth, subsequent creation of an access cavity with a dental handpiece, cleaning & shaping the root canals with an endodontic file, and restoration with gutta-percha filling and a crown

Removing infected pulp during a root canal procedure
Treatment procedure
The procedure is often complicated, depending on circumstances, and may involve multiple visits over a period of weeks.
Diagnostic and preparation

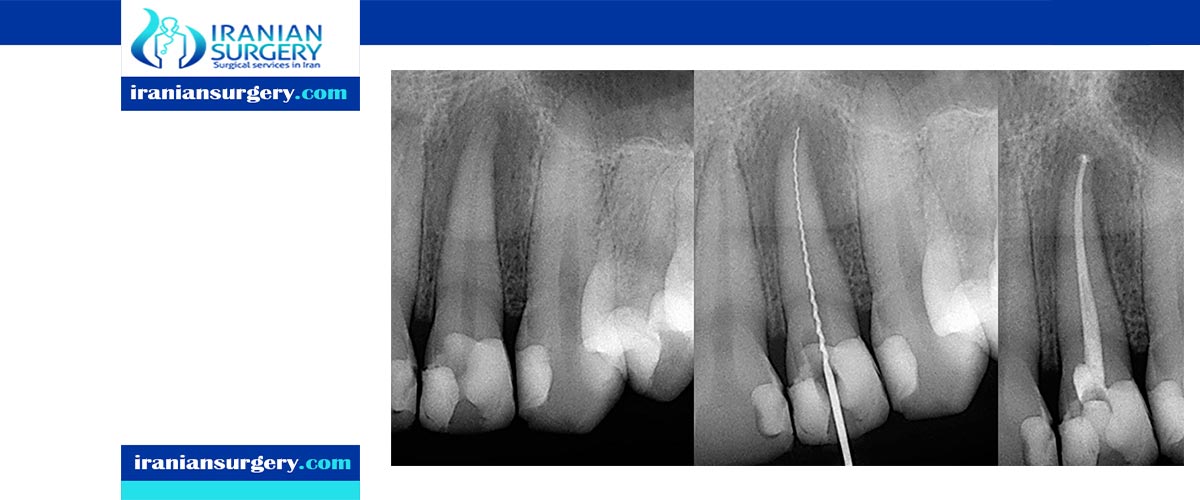
x-ray of a root canal operation

Tooth #13, the upper left second premolar, after excavation of DOdecay. There was a carious exposure into the pulp chamber (red oval), and the photo was taken after endodontic access was initiated and the roof of the chamber was removed.
Before endodontic therapy is carried out, a correct diagnosis of the dental pulp and the surrounding periapical tissues is required. This allows the endodontist to choose the most appropriate treatment option, allowing preservation and longevity of the tooth and surrounding tissues. Treatment options for an irreversibly inflamed pulp (irreversible pulpitis) include either extraction of the tooth or removal of the pulp.
Removing the infected/inflamed pulpal tissue enables the endodontist to help preserve the longevity and function of the tooth. The treatment option chosen involves taking into account the expected prognosis of the tooth, as well as the patient’s wishes. A full history is required (which includes the patient's symptoms and medical history), along with a clinical examination (both inside and outside the mouth), and the use of diagnostic tests
There are several diagnostic tests that can aid in the diagnosis of the dental pulp and the surrounding tissues. These include:
- Palpation (this is where the tip of the root is felt from the overlying tissues to see if there is any swelling or tenderness present)
- Mobility (this is assessing if there is more than normal movement of the tooth in the socket)
- Percussion (TTP, tender to percussion; the tooth is tapped to see if there is any tenderness)
- Transillumination (shining a light through the tooth to see if there are any noticeable fractures)
- Tooth slooth (this is where the patient is asked to bite down upon a plastic instrument; useful if the patient complains of pain on biting as this can be used to localise the tooth)
- Radiographs
- Dental pulp tests
In the situation that a tooth is considered so threatened (because of decay, cracking, etc.) that future infection is considered likely or inevitable, a pulpectomy (removal of the pulp tissue) is advisable to prevent such infection. Usually, some inflammation and/or infection is already present within or below the tooth. To cure the infection and save the tooth, the dentist drills into the pulp chamber and removes the infected pulp and then drills the nerve out of the root canal(s) with long needle-shaped hand instruments known as files (H files and K files).
Opening in the crown
The endodontist makes an opening through the enamel and dentin tissues of the tooth, usually using a dental drill fitted with a dental burr.
Isolating the tooth
The use of a rubber dam for tooth isolation is mandatory in endodontic treatment for several reasons:
- It provides an aseptic operating field, isolating the tooth from oral and salivary contamination. Root canal contamination with saliva introduces new microorganisms to the root canal which compromise the prognosis.
- It facilitates the use of the strong medicaments necessary to clean the root canal system.
- It protects the patient from the inhalation or ingestion of endodontic instruments.

Removal of pulp tissue
Procedures for shaping
There have been a number of progressive iterations to the mechanical preparation of the root canal for endodontic therapy. The first, referred to as the standardized technique, was developed by Ingle in 1961, and had disadvantages such as the potential for loss of working length and inadvertent ledging, zipping or perforation. Subsequent refinements have been numerous, and are usually described as techniques. These include the step-back, circumferential filing, incremental, anticurvature filing, step-down, double flare, crown-down-pressureless, balanced force, canal master, apical box, progressive enlargement, modified double flare, passive stepback, alternated rotary motions, and apical patency techniques.
The step back technique, also known as telescopic or serial root canal preparation, is divided in two phases: in the first, the working length is established and then the apical part of the canal is delicately shaped since a size 25 K-file reaches the working length; in the second, the remaining canal is prepared with manual or rotating instrumentation. This procedure, however, has some disadvantages, such as the potential for inadvertent apical transportation. Incorrect instrumentation length can occur, which can be addressed by the modified step back. Obstructing debris can be dealt with by the passive step back technique. The crown down is a procedure in which the dentist prepares the canal beginning from the coronal part after exploring the patency of the whole canal with the master apical file.
There is a hybrid procedure combining step back and crown down: after the canal's patency check, the coronal third is prepared with hand or Gates Glidden drills, then the working length is determined and finally the apical portion is shaped using step back techniques. The double flare is a procedure introduced by Fava where the canal is explored using a small file. Then canal is prepared in crown down manner using K-files then follows a "step back" preparation with 1 mm increments with increasing file sizes. With early coronal enlargement, also described as "three times technique", apical canals are prepared after a working length assessment using an apex locator; then progressively enlarged with Gates Glidden drills (only coronal and middle third). For the eponymic third time the dentist "arrives at the apex" and, if necessary, prepares the foramen with a size 25 K-file; the last phase is divided in two refining passages: the first with a 1-mm staggered instrument, the second with 0.5-mm staggering.[citation needed] From the early nineties engine-driven instrumentation were gradually introduced including the ProFile system, the Greater Taper files, the ProTaper files, and other systems like Light Speed, Quantec, K-3 rotary, Real World Endo, and the Hero 642.[citation needed]
All of these procedures involve frequent irrigation and recapitulation with the master apical file, a small file that reaches the apical foramen. High frequency ultrasound based techniques have also been described. These can be useful in particular for cases with complex anatomy, or for retained foreign body retrieval from a failed prior endodontic procedure.
Operative techniques for instruments
There are two slightly different anti-curvature techniques. In the balanced forces technique, the dentist inserts a file into the canal and rotates clockwise a quarter of a turn, engaging dentin, then rotates counter-clockwise half/ three-quarter of a revolution, applying pressure in an apical direction, shearing off tissue previously meshed. From the balanced forces stem two other techniques: the reverse balanced force (where GT instruments are rotated first anti-clockwise and then clockwise) and the gentler "feed and pull" where the instrument is rotated only a quarter of a revolution and moved coronally after an engagement, but not drawn out.
Irrigation
The root canal is flushed with an irrigant. The following substances may be used as root canal irrigants during the root canal procedure:
- Sodium hypochlorite (NaClO) in concentrations ranging between 0.5% and 5.25%
- 6% sodium hypochlorite with surface modifiers for better flow into nooks and crannies
- 2% chlorhexidine gluconate
- 0.2% chlorhexidine gluconate plus 0.2% cetrimide
- 17% ethylenediaminetetraacetic acid (EDTA)
- Framycetin sulfate
- Mixture of citric acid, doxycycline, and polysorbate 80 (detergent) (MTAD)
- Saline
- Absolute alcohol
The primary aim of chemical irrigation is to kill microbes and dissolve pulpal tissue. Certain irrigants, such as sodium hypochlorite and chlorhexidine, have proved to be effective antimicrobials in vitro and are widely used during root canal therapy worldwide. According to a systematic review, however, there is a lack of good quality evidence to support the use of one irrigant over another in terms of both short and long term prognosis of therapy.
Root canal irrigation systems are divided into two categories: manual agitation techniques and machine-assisted agitation techniques. Manual irrigation includes positive-pressure irrigation, which is commonly performed with a syringe and a side vented needle. Machine-assisted irrigation techniques include sonics and ultrasonics, as well as newer systems which deliver apical negative-pressure irrigation.
Filling the root canal
The standard filling material is gutta-percha, a natural polymer prepared from latex from the percha tree (Palaquium gutta). The standard endodontic technique involves inserting a gutta-percha cone (a "point") into the cleaned-out root canal along with a sealing cement.Another technique uses melted or heat-softened gutta-percha which is then injected or pressed into the root canal passage(s). However, since gutta-percha shrinks as it cools, thermal techniques can be unreliable and sometimes a combination of techniques is used. Gutta-percha is radiopaque, allowing verification afterwards that the root canal passages have been completely filled and are without voids.[citation needed]
An alternative filling material was invented in the early 1950s by Angelo Sargenti. Filling material has undergone several formulations over the years (N2, N2 Universal, RC-2B, RC-2B White), but all contain paraformaldehyde. The paraformaldehyde, when placed into the root canal, forms formaldehyde, which penetrates and sterilizes the passage. The formaldehyde is then theoretically transformed into harmless water and carbon dioxide. According to some research, the outcome of this method is better than a root canal procedure performed with gutta-percha. There is, however, a lack of indisputable scientific studies according to the Swedish Council on Health Technology Assessment.
alls of root canal and between the gutta-percha cones
In rare cases, the paste, like any other material, can be forced past the root tip into the surrounding bone. If this happens, the formaldehyde will immediately be transformed into a harmless substance. Blood normally contains 2 mg formaldehyde per liter and the body regulates this in seconds. The rest of an overfill will be gradually absorbed and the end result is normally good. In 1991, the ADA Council on Dental Therapeutics resolved that the treatment was "not recommended", and it is not taught in American dental schools. Scientific evidence in endodontic therapy was, and still is lacking. Despite this lack of support, the Sargenti technique has advocates who believe N2 to be less expensive and at least as safe as gutta-percha.
Pain control can be difficult to achieve at times because of anesthetic inactivation by the acidity of the abscess around the tooth apex. Sometimes the abscess can be drained, antibiotics prescribed, and the procedure reattempted when inflammation has been mitigated. The tooth can also be unroofed to allow drainage and help relieve pressure.
A root treated tooth may be eased from the occlusion as a measure to prevent tooth fracture prior to the cementation of a crown or similar restoration. Sometimes the dentist performs preliminary treatment of the tooth by removing all of the infected pulp of the tooth and applying a dressing and temporary filling to the tooth. This is called a pulpectomy. The dentist may also remove just the coronal portion of the dental pulp, which contains 90% of the nerve tissue, and leave intact the pulp in the canals. This procedure, called a "pulpotomy", tends to essentially eliminate all the pain. A pulpotomy may be a relatively definitive treatment for infected primary teeth. The pulpectomy and pulpotomy procedures aim to eliminate pain until the follow-up visit for finishing the root canal procedure. Further occurrences of pain could indicate the presence of continuing infection or retention of vital nerve tissue.[citation needed]
Some dentists may decide to temporarily fill the canal with calcium hydroxide paste in order to thoroughly sterilize the site. This strong base is left in place for a week or more to disinfect and reduce inflammation in surrounding tissue, requiring the patient to return for a second or third visit to complete the procedure. There appears to be no benefit from this multi-visit option, however, and single-visit procedures actually show better (though not statistically significant) patient outcomes than multi-visit ones.
Temporary filling
A temporary filling material is applied between the visits.Leaky temporary filling will allow the root canals to become reinfected by bacteria in the saliva (coronal microleakage). Khayat et al. showed that all root canals obturated with gutta-percha and root canal sealer using either lateral or vertical condensation were recontaminated in less than 30 days when exposed to saliva. Therefore, maintaining a coronal seal throughout root canal therapy is very important for the success of the treatment.
Final restoration
Molars and premolars that have had root canal therapy should be protected with a crown that covers the cusps of the tooth. This is because the access made into the root canal system removes a significant amount of tooth structure. Molars and premolars are the primary teeth used in chewing and will almost certainly fracture in the future without cuspal coverage. Anterior teeth typically do not require full coverage restorations after a root canal procedure, unless there is extensive tooth loss from decay or for esthetics or unusual occlusion. Placement of a crown or cusp-protecting cast gold covering is recommended also because these have the best ability to seal the treated tooth. There is insufficient evidence to assess the effects of crowns compared to conventional fillings for the restoration of root-filled teeth, decision of restoration should rely on the clinical experience of the practitioner and the preference of the patients. If the tooth is not perfectly sealed, the canal may leak, causing eventual failure. Also, many people believe once a tooth has had a root canal treatment it cannot further decay. This is not true, however: a tooth with a root canal treatment still has the ability to decay, and without proper home care and an adequate fluoride source the tooth structure can become severely decayed (often without the patient's knowledge since the nerve has been removed, leaving the tooth without any pain perception). Thus, non-restorable carious destruction is the main reason for extraction of teeth after root canal therapy, accounting for up to two-thirds of these extractions. Therefore, it is very important to have regular X-rays taken of the root canal to ensure that the tooth is not having any problems that the patient would not be aware of.[citation needed]
Endodontic retreatment
Endodontic treatment may fail for many reasons: one common reason for failure is inadequate chemomechanical debridement of the root canal. This may be due to poor endodontic access, missed anatomy or inadequate shaping of the canal, particularly in the apical third of the root canal, also due to the difficulty of reaching the accessory canals which are minute canals that extend in from the pulp to the periodontium in a random direction. They are mostly found in the apical third of the root.
Exposure of the obturation material to the oral environment may mean the gutta-percha is contaminated with oral bacteria. If complex and expensive restorative dentistry is contemplated then ideally the contaminated gutta percha would be replaced in a retreatment procedure to minimise the risk of failure.
The type of bacteria found within a failed canal may differ from the normal infected tooth. Enterococcus faecalis and/or other facultative enteric bacteria or Pseudomonas sp. are found in this situation.
Endodontic retreatment is technically demanding; it can be a time consuming procedure, as meticulous care is required by the dentist. Retreatment cases are typically referred to a specialist endodontist. Use of an operating microscope or other magnification may improve outcomes.
4 Comments
Why does teeth get infected after tooth canal?
Usually after this treatment, the tooth is maintained for a long time and works without any problems. Reinfection has a rare possibility, but there are reasons for this problem. The cause of a tooth infection may be wider than the dentist imagined, Either the root canal network may be much more complex than usual and some of the thinner channels may not be cleaned, or the protective crown may be punctured and allow the dental cavity to penetrate and re-infect the canal .If the tooth is re-infected after a root canal, it still does not mean that the tooth is gone. Another root treatment can be done to improve it. If you have been undergoing a root canal recently and have pain and swelling around the treated tooth, Symptoms of reinfection may be present and it is advisable to see your doctor promptly.
Does tooth decay harm pregnancy?
Pregnancy may make you more susceptible to infection, but that does not mean that pregnancy can cause these problems. If you already have problems with your tooth, these problems may be exacerbated during pregnancy. Some severe dental problems may require urgent medical care, such as dental implantation.