

Knee Osteotomy
What is Knee Osteotomy?
Knee osteotomy is a surgical procedure that your doctor might recommend if you have arthritis damage in just one area of your knee. Osteotomy is also performed in combination with other types of knee surgery, such as cartilage surgery, if your leg is bowed or knock-kneed.
The procedure involves removing or adding a wedge of bone to your shinbone (tibia) or thighbone (femur) to help shift your body weight off the damaged portion of your knee joint.
Knee osteotomy is most commonly performed on people who are younger than 60 who are active. Many people who undergo this procedure for arthritis might need a total knee replacement — usually about 10 to 15 years after the knee osteotomy.
Before Knee Osteotomy
Why it's done
Slick cartilage covers the ends of the bones in a healthy knee and this allows the bones to move smoothly against each other. Osteoarthritis damages and wears away the cartilage — creating a rough surface.
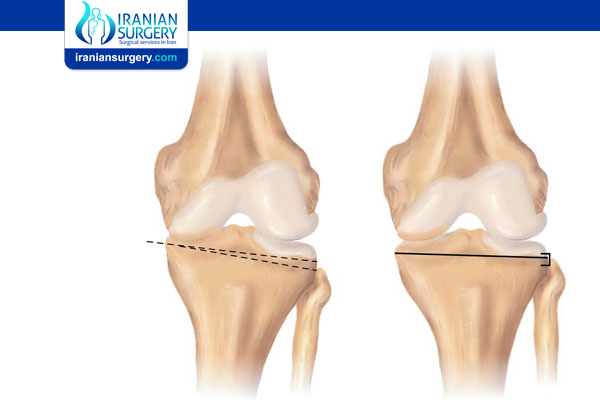
When the cartilage wears unevenly, it narrows the space between the femur and tibia, causing the knee to bow inward or outward, depending on which side of the knee is affected. Removing or adding a wedge of bone in your upper shinbone or lower thighbone can help straighten the bowing, shift your weight to the undamaged part of your knee joint and prolong the life span of the knee joint.
Who are the best candidates for Knee osteotomy?
Making sure the patient is a good candidate for surgery is important to help ensure a good outcome. Typically the best candidates:
. Have mild to moderate arthritis affecting only one side of the knee and little to no damage on the other side
. Are relatively young (40 to 60 years of age)
. Are not overweight
. Have good knee mobility
. Have significant arthritis pain that is brought on by activity or standing for an extended period of time
. Want to stay physically active and are willing to commit to a long post-surgical physical therapy regimen
. Are able to use crutches and limit weight bearing for 6 to 8 weeks after the surgery
People who elect to have osteotomy surgery tend to be physically active individuals who are motivated to stay active.
Read more about : Knee replacement
Knee Osteotomy Risks and Complications
The most common risks and complications are as follows:
. Any major surgery involving general anesthesia poses a low risk of strokes, heart attacks, pneumonia, and blood clots. Blood clots, or deep vein thrombosis (DVT), are the most common complication of knee osteotomy or knee replacement, but only affect a small percentage of patients.
. The surgical area can become infected. If the infection does not respond to antibiotics, another surgery or series of surgeries may be required.
. The peroneal nerve or blood vessels that runs down the back of the leg can be damaged during surgery. The peroneal nerve can also be damaged during recovery if the cast, brace or bandages are too constricting, putting too much pressure on the back of the knee for long periods of time.
. The bones at the osteotomy site may fail to grow together and heal.
. Osteotomy surgery may not provide pain relief. It is unlikely, but possible, that post-surgical pain will be worse than osteoarthritic pain.
. An under-correction or over-correction can result if the wedge of bone added or taken away was too small or too big. This means a knock-kneed person would become bowlegged or vice-versa.
. Because a wedge of bone has been added or taken away, a patient’s legs may be different lengths after surgery.
. Though the bones that comprise the knee joint may be better aligned, there can be complications involving the muscles, ligaments, and tendons that surround and support the joint. For example, a closed wedge tibial osteotomy can loosen the tension of the anterior cruciate ligament (ACL), which helps attach the tibia and femur.
Before electing to have knee osteotomy surgery, patients should talk to their surgeon about the potential risks and complications.
Potential Advantages and Disadvantages of Knee Osteotomy
For a select group of active knee arthritis patients under age 60, knee osteotomy is a reasonable surgical treatment option.
Pros:
. The potential advantages of knee osteotomy over knee replacement surgery are that:
. The actual knee joint, including ligaments, is preserved.
. Once healed, many patients can return to high-impact activities, such as jogging or playing basketball, which is not recommended after total knee replacements.
Cons:
Compared to total knee replacement, knee osteotomy has potential disadvantages, including that it:
. Requires more healing time
. Is more prone to complications
. Requires the patient to use crutches during bone healing
. Depends on successful bone healing, and there are many factors which regulate bone healing, not all of which are known or controlled
. Is less dependable for pain relief (and then a partial or total knee replacement may be recommended)
. Is not a cure for arthritis
. Does not replace the cartilage that is already lost or repair the remaining cartilage
In addition, an osteotomy usually just delays the need for a total knee replacement. Knee osteotomy results vary but typically last for about 10 years, at which time a knee replacement will likely be necessary.
Preparing for Knee Osteotomy Surgery
A patient may be asked to make several medical and home preparations to ensure a successful surgery and recovery
A doctor or nurse will provide the patient with a list of medical preparations that can help lower the risk of surgical and post-surgical complications. Certain medical preparations are required, while others are recommended.
. Medical Preparations for Knee Osteotomy
. Patients may be asked to wear a leg brace that mimics the knee alignment after an osteotomy. Wearing the brace for several days can help patients gauge whether knee osteotomy will be of benefit.
. Patients may be asked to spend time on an exercise bike or do other exercises that will help build strength and improve knee range of motion before surgery.
. Many doctors instruct patients to thoroughly wash the leg(s) each day in the week leading up to the surgery to decrease the chance of postoperative infection. Some doctors may even require patients to shower with a specific antiseptic, antimicrobial skin cleanser, such as Hibiclens, each day for 4 days prior to their surgeries.
. Patients should avoid sunburn, scrapes, poison ivy, and other problems that may negatively affect the skin around the surgical wound. Notify the surgeon of any of the above, as surgery may need to be rescheduled.
. Two weeks before surgery, a patient may be asked to stop taking certain medications, such as:
. Aspirin, NSAIDS (e.g. Aleve, Advil, any type of ibuprofen), and other medications that make it more difficult for blood to clot
. Steroids and other medications that suppress the immune system, and therefore, may increase the chance of post-surgical infection.
. A patient may also be told to eliminate smoking at least two weeks prior to surgery, as nicotine slows healing and increases the risk of deep vein thrombosis, a potentially deadly blood clot in a deep vein, after surgery.
. A patient who has other medical conditions, such as diabetes or heart disease, may be required to obtain medical clearance from his or her surgeon, primary care physician, or other doctor(s), verifying that the patient is healthy enough for surgery and anesthesia.
. Patients who have more than 1 or 2 alcoholic drinks per day should tell their doctors, as heavy alcohol use can impact the effects of anesthesia.
. Patients who get sick (cold, flu, fever, herpes breakout, etc.) in the days preceding a surgery should report it to the surgeon.
Patients who follow through with medical preparations improve the likelihood of a successful recovery.
. Home Preparations for Knee Osteotomy
Preparation will decrease stress and anxiety when arriving home. Household preparations will reduce the chance of falls, which can jeopardize a successful recovery.
. Arrange for a spouse, friend or other caregiver to provide meals and help around the house.
. Arrange for transportation, as most patients cannot drive for the first 6 to 8 weeks after surgery.
. Stock up on pre-made meals, canned food, and toiletry items to avoid having to run errands post-surgery.
. If possible, arrange to spend sleeping and waking hours on the same floor in order to avoid stairs. Also, adjust bed height (not too high or too low) to help ease getting in and out of bed, if possible.
. Take away or move anything that might be tripped over, such as area rugs or electrical cords.
. Make sure all stairs have sturdy railings.
. Install small rails or grab bars near toilets and in showers.
. Install a modified toilet seat. The higher seat will make it easier to sit down and get up and put less stress on the healing leg.
. Put a small stool in the shower to avoid standing on a slippery surface.
. Have a comfortable, supportive chair with an ottoman to keep the affected leg elevated for intervals.
. Consider practicing using walkers, canes, and other assistive devices ahead of time to ensure familiarity with them.
During Knee Osteotomy
Types of Knee Osteotomy Surgery
“Knee osteotomy” is a bit of a misnomer, because the knee joint itself, where the surfaces of the tibia (shin bone), femur (thigh bone) and patella (knee cap) meet, is not surgically altered. Rather, the alignment of the femur and tibia is adjusted.
Open or Closed Osteotomy
During surgery either the tibia or femur is cut from the side, and one of two types of osteotomy is performed.
. Closed osteotomy
A wedge of bone is cut and removed. The resulting gap in the bone is closed by bringing the two sides together and securing them with a plate and screws.
. Open osteotomy
A cut is made about three-quarters of the way across the bone. A wedge-shaped bone graft is inserted into the cut. The wedge is secured to the bone with a plate and screws. There are three types of bone graft–autograft, allograft, and artificial graft.
. Autograft. The inserted wedge is bone taken from another bone in the patient’s body, usually the pelvic bone, during the surgery.
. Allograft. The inserted wedge is bone from another person. Usually these grafts are procured from bone banks that harvest and freeze bone from cadavers.
. Artificial graft. The inserted wedge is made from a synthetic bone substitute.
Generally speaking, an autograft is the best option for post-surgical bone growth and healing, but some patients can have pain or other problems at the site where the bone was taken from the pelvis. What type of graft is used will be decided by the surgeon and patient.
A surgeon will make precise measurements regarding a patient’s leg alignment to determine whether to perform an osteotomy on the shin bone (tibia) or thigh bone (femur), decide which side of the bone to operate on, and calculate the exact size of the bone wedge to be added or removed for an osteotomy. How big of a wedge is added or removed depends on the person’s anatomy and degree of bow-legged or knock-kneed deformity. Typically, a 1 mm wedge will provide 1 degree of correction, so a 10 mm wedge will provide a 10-degree change in knee alignment.
The most common type of knee osteotomy is a high tibial medial opening wedge osteotomy, a surgery that adds a wedge of bone graft or substitute to the inner shin bone, just below the knee. It is typically done for bowlegged patients, relieving pressure on the inside of the knee and transferring it to the outside of the knee.
During the procedure
Knee Osteotomy Surgery Procedure Step-by-Step
Below is a step-by-step description of a typical high tibial osteotomy surgery. Other types of osteotomies to correct knee osteoarthritis will follow the same general steps. A typical knee osteotomy surgery takes about 90 minutes to complete.
. The patient’s vital signs are checked to make sure blood pressure, heart rate, body temperature, and oxygenation levels are normal and surgery can proceed. A mark is made on the knee undergoing surgery.
. Anesthesia is administered. Patients receive general anesthesia (are put to sleep) or are given a regional anesthesia to block sensation from the waist down along with a relaxant. General anesthesia is more common. The type of anesthesia a patient receives is decided well ahead of time.
. Before the osteotomy is done, the surgeon may check the knee joint to confirm that there is no significant cartilage damage on the “good side” of the knee. This can be done arthroscopically right before the osteotomy procedure.
. If a meniscal repair, microfracture surgery to promote cartilage growth, or other arthroscopic surgery is to be performed in addition to the osteotomy, the arthroscopic surgery will be done first.
. The surgeon will make a 4 to 5 inch incision in the skin. For a high tibial osteotomy this incision will be below the knee. The surgeon must then make incisions in deeper soft tissue, such as muscle, to expose the bone to be altered.
. The surgeon uses a bone saw to make a precise cut from one side of the bone and stops short about 1 cm before reaching the other side.
. In a closed osteotomy, another cut is made and a wedge of bone is removed. In an open osteotomy a wedge-shaped bone graft is inserted into the cut bone. The surgeon will use a tool to gently tap the wedge into place.
. The surgeon will double-check the new knee alignment and, if necessary, adjust the size of the wedge.
. The bone at the osteotomy wound is pushed together (e.g. pressure may be exerted on the flat of the foot), and the newly altered bone is secured with metal plates and screws.
. The surgeon will close up the surgical wound.
After Knee Osteotomy
Knee Osteotomy Recovery
Patients who have had knee osteotomy surgery will spend two or more days in the hospital. Because a bone has been intentionally broken, recovering patients will need to spend several weeks on crutches and commit to months of physical therapy or exercise. Patients will have regular follow-up visits with the surgeon’s office to monitor healing. Generally, patients will begin walking unaided 8 to 12 weeks post surgery. A complete recovery can range from 6 months to an entire year.
The timeline for rehabilitation varies significantly depending on the several variables, including:
. The size and location of the wedge of bone that was inserted or removed
. If the surgery was closed wedge (removing bone) or open wedge (inserting bone)
. If an open wedge osteotomy was performed, recovery time may also depend on what type of wedge was inserted. A bone graft from the patient (autograft) may take less time to heal than a bone graft from a donor or an artificial graft.
. The placement and type of hardware used to secure the osteotomy
. The patient’s overall health and ability to heal, possible surgical complications, and other factors.
Knee Osteotomy Recovery Goals and Priorities
Regardless of the exact timeline, a knee osteotomy recovery and rehabilitation program focuses on pain control, wound healing, protecting the osteotomy, improving flexibility and range of motion, and building muscle strength.
. Pain control. Recovery from knee osteotomy surgery is painful. Pain medication will be given in the hospital and prescribed for after discharge. If at any time pain is not being controlled well with medications, patients should talk to their doctor. Pain is easier to manage when it is addressed in its early stages.
. Soft tissue wound healing. While in the hospital, a patient will be taught how to care for the wound once he or she gets home, including changing bandages and bathing. Keeping the wound clean and free of infection is very important.
. Reduce swelling and prevent deep vein thrombosis. In the first two weeks following the surgery, steps must be taken to reduce swelling in the knee, avoid blood pooling in the leg veins and prevent Deep Vein Thrombosis (sometimes called DVT). The leg should be elevated, and ice packs may be used intermittently to reduce swelling. Two medical devices may be used: a Cryocuff and/or a Continuous Passive Motion Machine.
. Cryocuff. Some patients wear a “cryocuff,” a soft, puffy cast with a Velcro closure that has cold water circulating through it. The cold compression provided by the cryocuff helps reduce swelling. Patients also may be asked to contract and relax the thigh muscles and flex and point the ankle to promote blood flow in the leg.
. Continuous Passive Motion Machine (CPMM). Attached to a bed, a Continuous Passive Motion Machine is used while the patient is lying on his or her back. This machine keeps the leg elevated and gently moves the leg from a straight to bent position over and over again without the patient’s help. The Continuous Passive Motion Machine can help reduce swelling by keeping the leg elevated, reduce the chance of Deep Vein Thrombosis by keeping the leg moving, and facilitates flexibility and range of motion by forcing repeated bending and flexing.
. Protecting the osteotomy. Patients will wear a brace to help protect and support the leg. Bearing too much weight on the leg too soon after surgery could cause the bone at the osteotomy site to shift, upsetting the knee’s newly corrected alignment. Therefore, it is important for patients to carefully follow their doctors’ instructions. Some osteotomy patients are allowed partial weight bearing soon after surgery. Many other patients are told not to bear any weight on the leg for at least 6 weeks, when an x-ray can confirm the osteotomy is healing well.
Patients who are told to avoid weight-bearing activity will use crutches, keeping the affected leg completely off the floor. Once partial weight bearing is permitted, a doctor or physical therapist should give specific instructions about how to use crutches and perform exercises without putting too much weight on the leg.
. Improving flexibility and range of motion. The formation of fibrous scar tissue is part of the healing process, but too much scar tissue can impede the knee’s ability to completely straighten and flex. Scar tissue can also feel uncomfortable and lumpy under the skin. Knee stretching and flexing exercises will help prevent the buildup of scar tissue after surgery.
Typically, a doctor will want the patient to be able to be able bend the affected knee to at least a 90-degree angle and fully straighten it within 1 or 2 weeks after surgery. After several weeks of physical therapy, the knee should fully straighten and flex at least 135 degrees.
. Building muscle strength. As swelling decreases and the wound heals, priorities will shift to building muscle strength. Physical therapy will include various leg lifts and slowly integrate more challenging partial- and eventually full-weight bearing exercises, such as squats. Likewise, some patients may use a stationary bicycle, initially doing short rides of 5 to 10 minutes without any resistance and gradually building up to longer rides with some resistance.
While it may be tempting as the leg improves, patients should avoid any exercise that puts stress on the osteotomy wound without first having medical approval. Doing so may jeopardize the knee’s new alignment of the tibia, femur and patella (knee cap).
Most patients will still be using crutches and performing leg-straightening exercises at 8 weeks. It may take 3 to 6 months for osteotomy patients to walk normally and regain full range of motion. It may be 12 months or more before patients can participate in high impact activities, such as jogging.
Results
In most cases, knee osteotomy relieves arthritis pain and postpones the need for a total knee replacement by 10 to 15 years.
Knee Osteotomy vs. Knee Replacement
Knee osteotomy has become more common as the surgery has improved and surgical treatments for knee arthritis are more frequently used. The two primary reasons patients choose to have a knee osteotomy is that it preserves the natural tissue surrounding the knee and that it may postpone or eliminate the need for a knee replacement.
A knee osteotomy allows the actual knee joint—where the tibia, femur and patella (kneecap) meet—and all of the knee’s ligaments, to remain intact. Conserving the knee optimizes joint function and preserves the natural feeling of the knee throughout a full range of motion. These factors can be important to patients who want to continue to do activities that require higher levels of knee function, such as running, squatting, kneeling, and climbing.
A knee osteotomy may eliminate or postpone the need for knee replacement surgery. Postponing knee replacement surgery is important to some patients, because while the typical artificial knee lasts 15 years or more, it eventually may require a second surgery called a revision knee replacement surgery. Logically, patients want to make choices that will help them avoid the need for a revision knee replacement.
Knee Osteotomy Cost
The cost of Knee Osteotomy in Iran is about $ 2000.
Sources:
. https://www.arthritis-health.com/surgery/knee-surgery/knee-osteotomy-surgery
. https://www.mayoclinic.org/tests-procedures/knee-osteotomy/about/pac-20394514