

Biliopancreatic diversion with duodenal switch reversal
Biliopancreatic diversion with duodenal switch reversal
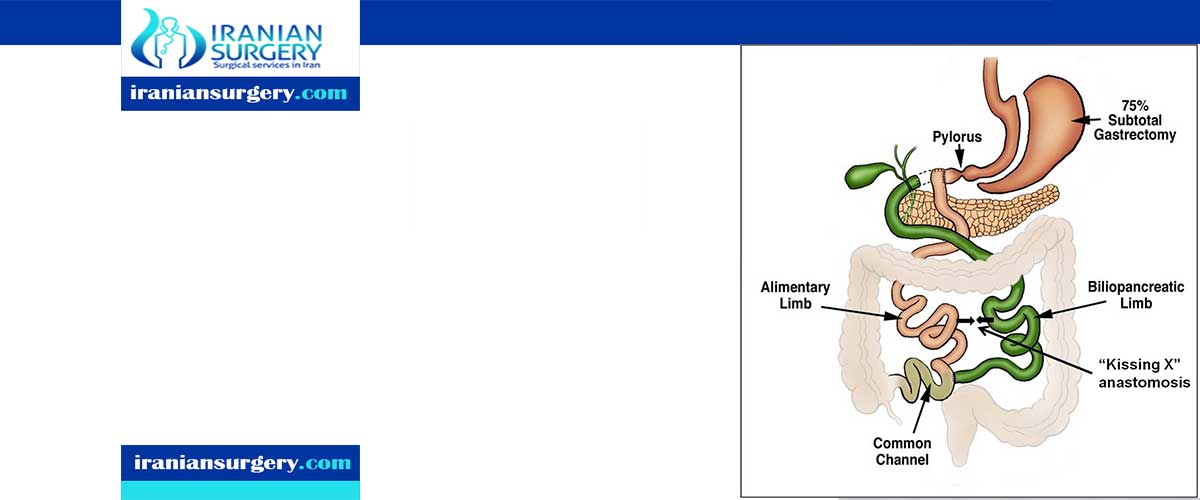
Biliopancreatic Diversion (BPD) creates a smaller stomach (similar to gastric bypass surgery), but in addition there is less absorption of ingested food inside the intestine (malabsorption).
Biliopancreatic diversion changes the normal process of digestion by making the stomach smaller and allowing food to bypass part of the small intestine so that patients absorb fewer calories. A portion of the stomach is removed entirely, creating a smaller stomach pouch. The distal part of the small intestine is then connected to the pouch. Like gastric bypass surgery, this type of operation has the potential for developing nutritional deficiencies.

Biliopancreatic diversion is a powerful bariatric procedure that relies on gastric restriction combined with a large malabsorptive component. This can lead to excessive side effects and/or weight loss. Despite this, long-term weight regain can also occur. Objectives: To determine the rate of and options for revision in patients who experience excessive side effects and weight loss. To explore the revisional procedures available to overcome weight regain. Methods: A PubMed search was conducted of all reports published between 1979 and August 31, 2014. Series and case reports on revision or reversal after biliopancreatic diversion with duodenal switch (BPD/DS) or without (BPD) were included. Results: Revision rates for excessive malabsorption ranges from .5%-4.9% and 3%-18.5% after BPD/DS and BPD respectively. Revisions increase common channel by up to 150 cm. Reversal is necessary in .2%-7% of cases, with an increased risk when the common channel is≤50 cm. In most instances, reversal (of the malabsorptive component only) is indicated after the revision failure. A proximal, side-to-side anastomosis between the biliopancreatic and alimentary limbs is the preferred option. Most reoperations are performed within 2 years of the initial procedure and for protein malnutrition in about half of the cases. Revision for insufficient weight loss is reported in .5%-2.78% of cases. Except inadequate channel lengths, little is to be gained by common channel shortening. Additional gastric restriction, which results in an average 9-14 kg weight loss, is another option. Conclusions: Biliopancreatic diversion can be relatively easily revised to control excessive side effects and protein malnutrition. Early diagnosis is essential and warrants a close nutritional monitoring. In case of weight regain, limited results can be obtained by reducing the gastric volume provided the lengths of the small bowel channels are adequate.
[kkstarratings]