

Benign prostatic hyperplasia
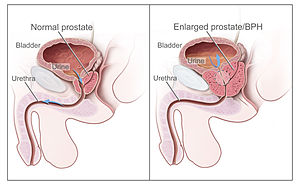
Benign prostatic hyperplasia (BPH), also called prostate enlargement, is a noncancerous increase in size of the prostate. Symptoms may include frequent urination, trouble starting to urinate, weak stream, inability to urinate, or loss of bladder control. Complications can include urinary tract infections, bladder stones, and chronic kidney problems.
The cause is unclear. Risk factors include a family history, obesity, type 2 diabetes, not enough exercise, and erectile dysfunction. Medications like pseudoephedrine, anticholinergics, and calcium channel blockers may worsen symptoms. The underlying mechanism involves the prostate pressing on the urethra thereby making it difficult to pass urine out of the bladder. Diagnosis is typically based on symptoms and examination after ruling out other possible causes.
Treatment options including lifestyle changes, medications, a number of procedures, and surgery. In those with mild symptoms weight loss, exercise, and decreasing caffeine intake is recommended. In those with more significant symptoms medications may include alpha blockers such as terazosin or 5α-reductase inhibitors such as finasteride. Surgical removal of part of the prostate may be carried out in those who do not improve with other measures. Alternative medicine, such as saw palmetto, does not appear to help.
About 105 million people are affected globally. BPH typically begins after the age of 40. Half of males age 50 and over are affected. After the age of 80 about 90% of males are affected. Although prostate specific antigen levels may be elevated in males with BPH, the condition does not increase the risk of prostate cancer.
Signs and symptoms
.png)
BPH is the most common cause of lower urinary tract symptoms (LUTS), which are divided into storage, voiding, and symptoms which occur after urination. Storage symptoms include the need to urinate frequently, waking at night to urinate, urgency (compelling need to void that cannot be deferred), involuntary urination, including involuntary urination at night, or urge incontinence (urine leak following a strong sudden need to urinate). Voiding symptoms include urinary hesitancy (a delay between trying to urinate and the flow actually beginning), intermittency (not continuous), involuntary interruption of voiding, weak urinary stream, straining to void, a sensation of incomplete emptying, and uncontrollable leaking after the end of urination. These symptoms may be accompanied by bladder pain or pain while urinating, called dysuria.
Bladder outlet obstruction (BOO) can be caused by BPH. Symptoms are abdominal pain, a continuous feeling of a full bladder, frequent urination, acute urinary retention (inability to urinate), pain during urination (dysuria), problems starting urination (urinary hesitancy), slow urine flow, starting and stopping (urinary intermittency), and nocturia.
BPH can be a progressive disease, especially if left untreated. Incomplete voiding results in residual urine or urinary stasis, which can lead to an increased risk of urinary tract infection.
Causes
Hormones
Most experts consider androgens (testosterone and related hormones) to play a permissive role in the development of BPH. This means that androgens must be present for BPH to occur, but do not necessarily directly cause the condition. This is supported by evidence suggesting that castrated boys do not develop BPH when they age. In an unusual study of 26 eunuchs from the palace of the Qing dynasty still living in Beijing in 1960, the prostate could not be felt in 81% of the studied eunuchs. The average time since castration was 54 years (range, 41–65 years). On the other hand, some studies suggest that administering exogenous testosterone is not associated with a significant increase in the risk of BPH symptoms, so the role of testosterone in prostate cancer and BPH is still unclear. Further randomized controlled trials with more participants are needed to quantify any risk of giving exogenous testosterone.
Dihydrotestosterone (DHT), a metabolite of testosterone, is a critical mediator of prostatic growth. DHT is synthesized in the prostate from circulating testosterone by the action of the enzyme 5α-reductase, type 2. DHT can act in an autocrine fashion on the stromal cells or in paracrine fashion by diffusing into nearby epithelial cells. In both of these cell types, DHT binds to nuclear androgen receptors and signals the transcription of growth factors that are mitogenic to the epithelial and stromal cells. DHT is ten times more potent than testosterone because it dissociates from the androgen receptor more slowly. The importance of DHT in causing nodular hyperplasia is supported by clinical observations in which an inhibitor of 5α-reductase such as finasteride is given to men with this condition. Therapy with a 5α-reductase inhibitor markedly reduces the DHT content of the prostate and, in turn, reduces prostate volume and BPH symptoms.
Testosterone promotes prostate cell proliferation, but relatively low levels of serum testosterone are found in patients with BPH. One small study has shown that medical castration lowers the serum and prostate hormone levels unevenly, having less effect on testosterone and dihydrotestosterone levels in the prostate.
While there is some evidence that estrogen may play a role in the cause of BPH, this effect appears to be mediated mainly through local conversion of androgens to estrogen in the prostate tissue rather than a direct effect of estrogen itself. In canine in vivo studies castration, which significantly reduced androgen levels but left estrogen levels unchanged, caused significant atrophy of the prostate. Studies looking for a correlation between prostatic hyperplasia and serum estrogen levels in humans have generally shown none.
In 2008, Gat et al. published evidence that BPH is caused by failure in the spermatic venous drainage system resulting in increased hydrostatic pressure and local testosterone levels elevated more than 100 fold above serum levels. If confirmed, this mechanism explains why serum androgen levels do not seem to correlate with BPH and why giving exogenous testosterone would not make much difference.
Diet
Studies indicate that dietary patterns may affect development of BPH, but further research is needed to clarify any important relationship. Studies from China suggest that greater protein intake may be a factor in development of BPH. Men older than 60 in rural areas had very low rates of clinical BPH, while men living in cities and consuming more animal protein had a higher incidence. On the other hand, a study in Japanese-American men in Hawaii found a strong negative association with alcohol intake, but a weak positive association with beef intake.In a large prospective cohort study in the US (the Health Professionals Follow-up Study), investigators reported modest associations between BPH (men with strong symptoms of BPH or surgically confirmed BPH) and total energy and protein, but not fat intake. There is also epidemiological evidence linking BPH with metabolic syndrome (concurrent obesity, impaired glucose metabolism and diabetes, high triglyceride levels, high levels of low-density cholesterol, and hypertension).
Degeneration
Benign prostatic hyperplasia is an age-related disease. Misrepair-accumulation aging theory suggests that development of benign prostatic hyperplasia is a consequence of fibrosis and weakening of the muscular tissue in the prostate. The muscular tissue is important in the functionality of the prostate, and provides the force for excreting the fluid produced by prostatic glands. However, repeated contractions and dilations of myofibers will unavoidably cause injuries and broken myofibers. Myofibers have a low potential for regeneration; therefore, collagen fibers need to be used to replace the broken myofibers. Such misrepairs make the muscular tissue weak in functioning, and the fluid secreted by glands cannot be excreted completely. Then, the accumulation of fluid in glands increases the resistance of muscular tissue during the movements of contractions and dilations, and more and more myofibers will be broken and replaced by collagen fibers.
Pathophysiology

Benign prostate hyperplasia
As men age, the enzymes aromatase and 5-alpha reductase increase in activity. Aromatase and 5-alpha reductase are responsible for converting androgen hormones into estrogen and dihydrotestosterone, respectively. This metabolism of androgen hormones leads to a decrease in testosterone but raised levels of DHT and estrogen.
Both the glandular epithelial cells and the stromal cells (including muscular fibers) undergo hyperplasia in BPH. Most sources agree that of the two tissues, stromal hyperplasia predominates, but the exact ratio of the two is unclear.
Anatomically the median and lateral lobes are usually enlarged, due to their highly glandular composition. The anterior lobe has little in the way of glandular tissue and is seldom enlarged. (Carcinoma of the prostate typically occurs in the posterior lobe – hence the ability to discern an irregular outline per rectal examination). The earliest microscopic signs of BPH usually begin between the age of 30 and 50 years old in the PUG, which is posterior to the proximal urethra. In BPH, the majority of growth occurs in the transition zone (TZ) of the prostate. In addition to these two classic areas, the peripheral zone (PZ) is also involved to a lesser extent.Prostatic cancer typically occurs in the PZ. However, BPH nodules, usually from the TZ are often biopsied anyway to rule out cancer in the TZ.
Diagnosis
The clinical diagnosis of BPH is based on a history of LUTS (lower urinary tract symptoms), a digital rectal exam, and exclusion of other causes of similar signs and symptoms. The degree of LUTS does not necessarily correspond to the size of the prostate. An enlarged prostate gland on rectal examination that is symmetric and smooth supports a diagnosis of BPH. However, if the prostate gland feels asymmetrical, firm, or nodular, this raises concern for prostate cancer.
Urinalysis is typically performed when LUTS are present and BPH is suspected to evaluate for signs of a urinary tract infection, glucose in the urine (suggestive of diabetes), or protein in the urine (suggestive of kidney disease). Bloodwork including kidney function tests and prostate specific antigen (PSA) are often ordered to evaluate for kidney damage and prostate cancer, respectively. However, checking blood PSA levels for prostate cancer screening is controversial and not necessarily indicated in every evaluation for BPH. Benign prostatic hyperplasia and prostate cancer are both capable of increasing blood PSA levels and PSA elevation is unable to differentiate these two conditions well. If PSA levels are checked and are high, then further investigation is warranted. Measures including PSA density, free PSA, rectal examination, and transrectal ultrasonography may be helpful in determining whether a PSA increase is due to BPH or prostate cancer. Ultrasound examination of the testes, prostate, and kidneys is often performed, again to rule out cancer and hydronephrosis.
Validated questionnaires such as the American Urological Association Symptom Index (AUA-SI), the International Prostate Symptom Score (I-PSS), and more recently the UWIN score (urgency, weak stream, incomplete emptying, and nocturia) are useful aids to making the diagnosis of BPH and quantifying the severity of symptoms.
Differential diagnosis
Medical conditions
The differential diagnosis for LUTS is broad and includes various medical conditions, neurologic disorders, and other diseases of the bladder, urethra, and prostate such as bladder cancer, urinary tract infection, urethral stricture, urethral calculi (stones), chronic prostatitis, and prostate cancer. Neurogenic bladder can cause urinary retention and cause symptoms similar to those of BPH. This may occur as a result of uncoordinated contraction of the bladder muscle or impairment in the timing of bladder muscle contraction and urethral sphincter relaxation. Notable causes of neurogenic bladder include disorders of the central nervous system such as Parkinson’s disease, multiple sclerosis, and spinal cord injuries as well as disorders of the peripheral nervous system such as diabetes mellitus, vitamin B12 deficiency, and alcohol-induced nerve damage. Individuals affected by heart failure often experience nighttime awakenings to urinate due to redistribution of fluid accumulated in swollen legs.
Medications
Certain medications can increase urination difficulties by increasing bladder outlet resistance by increasing smooth muscle tone at the prostate or bladder neck and contribute to LUTS. Alpha-adrenergic agonist medications, such as decongestants with pseudoephedrine can increase bladder outlet resistance. In contrast, calcium channel blockers and anticholinergic medications can worsen urinary retention by promoting bladder muscle relaxation. Diuretic medications such as loop diuretics (e.g., furosemide) or thiazides (e.g., chlorthalidone) can cause or worsen urinary frequency and nighttime awakenings to urinate.
-

Micrograph showing nodular hyperplasia (left off center) of the prostate from a transurethral resection of the prostate(TURP). H&E stain.
-

Microscopic examination of different types of prostate tissues (stained with immunohistochemicaltechniques): A. Normal (non-neoplastic) prostatic tissue (NNT). B. Benign prostatic hyperplasia. C. High-grade prostatic intraepithelial neoplasia(PIN). D. Prostatic adenocarcinoma (PCA).


Management
Lifestyle
Lifestyle alterations to address the symptoms of BPH include physical activity, decreasing fluid intake before bedtime, moderating the consumption of alcohol and caffeine-containing products and following a timed voiding schedule. Patients can also attempt to avoid products and medications with anticholinergic properties that may exacerbate urinary retention symptoms of BPH, including antihistamines, decongestants, opioids, and tricyclic antidepressants; however, changes in medications should be done with input from a medical professional.
Voiding position
Voiding position when urinating may influence urodynamic parameters (urinary flow rate, voiding time, and post-void residual volume). A meta-analysis found no differences between the standing and sitting positions for healthy males, but that, for elderly males with lower urinary tract symptoms, voiding in the sitting position:
- decreased the post void residual volume
- increased the maximum urinary flow, comparable with pharmacological intervention
- decreased the voiding time
This urodynamic profile is associated with a lower risk of urologic complications, such as cystitis and bladder stones.
Medications
The two main medication classes for BPH management are alpha blockers and 5α-reductase inhibitors.
Alpha blockers
Selective α1-blockers are the most common choice for initial therapy. They include alfuzosin, doxazosin, silodosin, tamsulosin, and terazosin. They have a small to moderate benefit. All five are equally effective but have slightly different side effect profiles. Alpha blockers relax smooth muscle in the prostate and the bladder neck, thus decreasing the blockage of urine flow. Common side effects of alpha blockers include orthostatic hypotension (a head rush or dizzy spell when standing up or stretching), ejaculation changes, erectile dysfunction, headaches, nasal congestion, and weakness.
Tamsulosin and silodosin are selective α1 receptor blockers that preferentially bind to the α1A receptor in the prostate instead of the α1B receptor in the blood vessels. Less-selective α1 receptor blockers such as terazosin and doxazosin may lower blood pressure. The older, less selective α1-adrenergic blocker prazosin is not a first line choice for either high blood pressure or prostatic hyperplasia; it is a choice for patients who present with both problems at the same time. The older, broadly non-selective alpha blocker medications such as phenoxybenzamine are not recommended for control of BPH. Non-selective alpha blockers such as terazosin and doxazosin may also require slow dose adjustments as they can lower blood pressure and cause syncope (fainting) if the response to the medication is too strong.
5α-Reductase inhibitors
The 5α-reductase inhibitors finasteride and dutasteride may also be used in men with BPH. These medications inhibit the 5α-reductase enzyme, which, in turn, inhibits production of DHT, a hormone responsible for enlarging the prostate. Effects may take longer to appear than alpha blockers, but they persist for many years. When used together with alpha blockers, no benefit was reported in short-term trials, but in a longer term study (3–4 years) there was a greater reduction in BPH progression to acute urinary retention and surgery than with either agent alone, especially in people with more severe symptoms and larger prostates. Other trials have confirmed reductions in symptoms, within 6 months in one trial, an effect that was maintained after withdrawal of the alpha blocker. Side effects include decreased libido and ejaculatory or erectile dysfunction. The 5α-reductase inhibitors are contraindicated in pregnant women because of their teratogenicity due to interference with fetal testosterone metabolism, and as a precaution, pregnant women should not handle crushed or broken tablets.
Others
Antimuscarinics such as tolterodine may also be used, especially in combination with alpha blockers. They act by decreasing acetylcholine effects on the smooth muscle of the bladder, thus helping control symptoms of an overactive bladder.
Phosphodiesterase-5 inhibitors such as sildenafil citrate show some symptomatic relief, suggesting a possible common cause with erectile dysfunction. Tadalafil was considered then rejected by NICE in the UK for the treatment of symptoms associated with BPH. In 2011, the U.S. Food and Drug Administration approved tadalafil to treat the signs and symptoms of benign prostatic hyperplasia, and for the treatment of BPH and erectile dysfunction (ED), when the conditions occur simultaneously.
Self-catheterization
Intermittent urinary catheterization is used to relieve the bladder in people with urinary retention. Self-catheterization is an option in BPH when it is difficult or impossible to completely empty the bladder.Urinary tract infection is the most common complication of intermittent catheterization. Several techniques and types of catheter are available, including sterile (single-use) and clean (multiple use) catheters, but, based on current information, none is superior to others in reducing the incidence of urinary tract infection.
Surgery

Prostate with a large median lobe bulging upwards. A metal instrument is placed in the urethra (which passes through the prostate). This specimen was almost 7 centimeters long with a volume of about 60 cubic centimeters on transrectal ultrasound and was removed during a Hryntschak procedure or transvesical prostatectomy (removal of the prostate through the bladder) for benign prostatic hyperplasia.
If medical treatment is not effective a person may try office-based therapies or transurethral resection of prostate (TURP), surgery may need to be performed. Surgical techniques used include the following:
- Open prostatectomy: not usually performed nowadays, even if results are very good.
- Transurethral resection of the prostate (TURP): the gold standard.
- Transurethral incision of the prostate (TUIP): rarely performed; the technique is similar to TURP but less definitive.
- Photoselective (laser) vaporization of the prostate (PVP): common treatment.
Endovascular
The latest alternative to surgical treatment is arterial embolization, an endovascular procedure performed in interventional radiology. Through catheters, embolic agents are released in the main branches of the prostatic artery, in order to induce a decrease in the size of the prostate gland, thus reducing the urinary symptoms.
Alternative medicine
While herbal remedies are commonly used, a 2016 review found them to be no better than placebo. Saw palmetto extract from Serenoa repens, while one of the most commonly used, is no better than placebo in both symptom relief and decreasing prostate size. Other herbal medicines include beta-sitosterol from Hypoxis rooperi (African star grass) and pygeum (extracted from the bark of Prunus africana), while there is less substantial support for the efficacy of pumpkin seed (Cucurbita pepo) and stinging nettle (Urtica dioica) root. A systematic review of Chinese herbal medicines found that the quality of studies was insufficient to indicate any superiority over Western medicines.
Epidemiology

Disability-adjusted life year for benign prostatic hyperplasia per 100,000 inhabitants in 2004.
Globally, benign prostatic hyperplasia affects about 210 million males as of 2010 (6% of the population).
The prostate gets larger in most men as they get older. For a symptom-free man of 46 years, the risk of developing BPH over the next 30 years is 45%. Incidence rates increase from 3 cases per 1000 man-years at age 45–49 years, to 38 cases per 1000 man-years by the age of 75–79 years. While the prevalence rate is 2.7% for men aged 45–49, it increases to 24% by the age of 80 years.
References
^ Jump up to:a “Prostate Enlargement (Benign Prostatic Hyperplasia)”. NIDDK. September 2014. Archivedfrom the original on 4 October 2017. Retrieved 19 October 2017.
- ^ Jump up to:Kim, EH; Larson, JA; Andriole, GL (2016). “Management of Benign Prostatic Hyperplasia”. Annual Review of Medicine (Review). 67: 137–51. doi:10.1146/annurev-med-063014-123902. PMID 26331999.
- ^ Jump up to:a b GBD 2015 Disease and Injury Incidence and Prevalence, Collaborators. (8 October 2016). “Global, regional, and national incidence, prevalence, and years lived with disability for 310 diseases and injuries, 1990–2015: a systematic analysis for the Global Burden of Disease Study 2015”. Lancet. 388 (10053): 1545–1602. doi:10.1016/S0140-6736(16)31678-6. PMC 5055577. PMID 27733282.
- https://en.wikipedia.org/wiki/Benign_prostatic_hyperplasia
[kkstarratings]