

Dilation and curettage
Dilation (or dilatation) and curettage (D&C) refers to the dilation (widening/opening) of the cervix and surgical removal of part of the lining of the uterus and/or contents of the uterus by scraping and scooping (curettage). It is a therapeutic gynecological procedure as well as the most often used method of first trimester miscarriage or abortion.
D&C normally refers to a procedure involving a curette, also called sharp curettage. However, some sources use the term D&C to refer more generally to any procedure that involves the processes of dilation and removal of uterine contents, which includes the more common suction curettage procedures of manual and electric vacuum aspiration.
Procedure
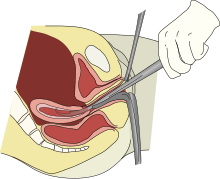
An illustration of a dilation and curettage
The woman is typically put under monitored anesthesia care (MAC) before the procedure begins. The first step in a D&C is to dilate the cervix. This can be done with Hegar dilators. A curette, a metal rod with a handle on one end and a sharp loop on the other, is then inserted into the uterus through the dilated cervix. The curette is used to gently scrape the lining of the uterus and remove the tissue in the uterus. This tissue is examined for completeness (in the case of abortion or miscarriage treatment) or by pathology for abnormalities (in the case of treatment for abnormal bleeding).
Clinical uses
D&Cs are commonly performed for the diagnosis of gynecological conditions leading to ‘abnormal uterine bleeding’; to resolve abnormal uterine bleeding (too much, too often or too heavy a menstrual flow); to remove the excess uterine lining in women who have conditions such as polycystic ovary syndrome (which cause a prolonged buildup of tissue with no natural period to remove it); to remove tissue in the uterus that may be causing abnormal vaginal bleeding, including postpartum retained placenta; to remove retained tissue (also known as retained POC or retained products of conception) in the case of a missed or incomplete miscarriage (in which some of the tissue remains in the uterus and the cervix stays open. This may increase a woman’s risk of infection and continued bleeding); and as a method of abortion. In contrast, D&C remains ‘standard care’ for missed and incomplete miscarriage in many countries despite the existence of alternatives currently used for abortions.
Because medicinal and non-invasive methods of abortion now exist, and because D&C requires heavy sedation or general anesthesia and has higher risks of complication, the procedure has been declining as a method of abortion. The World Health Organization recommends D&C as a method of surgical abortion only when manual vacuum aspiration is unavailable. Most D&Cs are now carried out for miscarriage management and other indications such as diagnosis.
Hysteroscopy is a valid alternative to D&C for many surgical indications from diagnosis of uterine pathology to the removal of fibroids and even retained products of conception. It poses less risk because the doctor has a view inside the uterus during surgery, unlike with blind D&C.
Medical management of miscarriage and medical abortion using drugs such as misoprostol and mifepristone are safe, non-invasive and cheaper alternatives to D&C.
Complications
Complications may arise from either the introduction or spreading of infection, adverse reaction to general anesthesia required during the surgery or from instrumentation itself, if the procedure is performed blindly (without the use of any imaging technique such as ultrasound or hysteroscopy).
One risk of sharp curettage is uterine perforation. Although normally no treatment is required for uterine perforation, a laparoscopy may be done to verify that bleeding has stopped on its own. Infection of the uterus or fallopian tubes is also a possible complication, especially if the woman has an untreated sexually transmitted infection.
Another risk is intrauterine adhesions, or Asherman’s syndrome. One study found that in women who had one or two sharp curettage procedures for miscarriage, 14-16% developed some adhesions. Women who underwent three sharp curettage procedures for miscarriage had a 32% risk of developing adhesions. The risk of Asherman’s syndrome was found to be 30.9% in women who had D&C following a missed miscarriage, and 25% in those who had a D&C 1–4 weeks postpartum. Untreated Asherman’s syndrome, especially if severe, also increases the risk of complications in future pregnancies, such as ectopic pregnancy, miscarriage, and abnormal placentation (e.g.placenta previa and placenta accreta). According to recent case reports, use of vacuum aspiration can also lead to intrauterine adhesions. Yet, in terms of long-term reproductive outcome after miscarriage, a review in 2013 came to the conclusion that there were no studies reporting a link to D&C, while similar pregnancy outcomes were reported subsequent to surgical management (including D&C), medical management or conservative management (that is, watchful waiting). After miscarriage, there is an association between surgical intervention in the uterus and the development of intrauterine adhesions, and between intrauterine adhesions and adverse pregnancy outcomes, but there is still no clear evidence of any method of prevention of adverse pregnancy outcomes related to intrauterine adhesions.
Reference:
https://en.wikipedia.org/wiki/Dilation_and_curettage
[kkstarratings]